Conceptual models for health impact assessment
We focused on conceptual epidemiological and health impact assessment models where we introduced half-life decays in calculating cumulative exposure. The half-life decays refer to applying weighting factors to gradually decrease the contribution of exposures that are more chronologically distant (i.e. occurred longer in the past). Within a pooled lung cancer case-control population (SYNERGY), we then used these decay-adjusted cumulative exposures (DACE) in epidemiological and HIA models to assess the effect of introducing various decay values in calculating cumulative exposures for six lung carcinogens. Finally, we proposed various criteria for determining appropriate decay values for the different exposures.
Key results
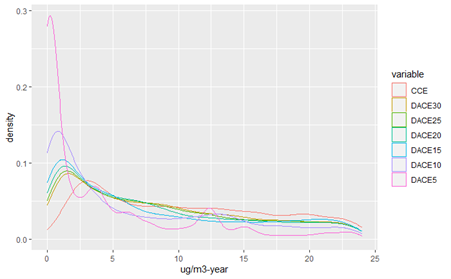
The distribution of cumulative exposure values in the SYNERGY study population changed with the application of various decay half-lives to exposure. Increasingly rapid exposure decay (i.e. shorter half-lives) led to larger changes in exposure distribution, shifting the distribution towards zero (Fig. 1).

Figure 1. Density plot of cumulative exposures with various decay values for diesel engine exhaust among exposed subjects in the SYNERGY population (truncated at 25th percentile CCE to highlight changes in lower cumulative exposures). CCE = conventional cumulative exposure; DACE = decay-adjusted cumulative exposure.
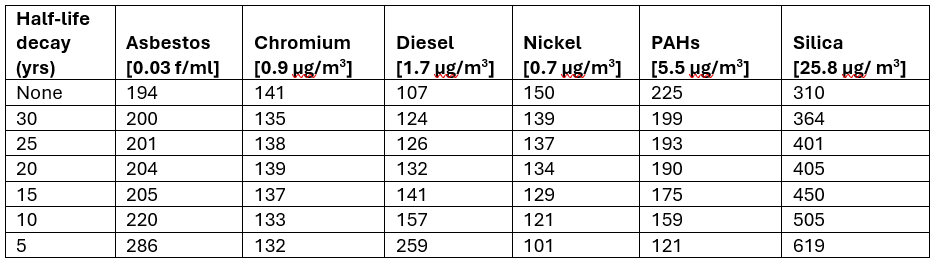
The application of exposure decays in lifetable analysis produced different results for different exposures (Table 1). With more rapid exposure decays, ELR estimates increased for asbestos, diesel, and silica and decreased for nickel and PAHs. ELRs for chromium were similar across the range of exposure decays tested.

Table 1: Excess lifetime risks of lung cancer mortality per 100,000 persons for SYNERGY exposures based on specified exposure scenario [in brackets] and various half-life decay values
Key conclusion and proposal:
We propose propose three sets of criteria, ranging from the most stringent to the least, to determine whether to apply DACE to an exposure:
- Model with lowest AIC with significant model fit improvement in the DACE model versus standard CCE model (AIC reduction >2), plus significant exposure cessation effect in the negative direction (p<0.05);
- Model with lowest AIC with suggestive model fit improvement in the DACE model versus standard model (AIC reduction >1), plus suggestive exposure cessation effect in the negative direction (P<0.1);
- Model with lowest AIC with any model fit improvement the DACE model versus standard model (AIC reduction >0), plus any exposure cessation effect in the negative direction.
For instance, from the SYNERGY dataset, no DACE model would be selected over the standard CCE model based on the most stringent set of criteria. For the next set of criteria, the silica DACE15 and chromium DACE10 models would be selected based on suggestive statistical evidence for improved model fit and cessation effect. In the least stringent set of criteria, the nickel DACE20 and asbestos DACE10 models would be added to the selection. In our health impact assessment models, compared to estimates with the standard CCE approach, ELRs from the selected DACE models would be 45% higher for silica, 6% lower for chromium, 11% lower for nickel, and 13% higher for asbestos.
{kind=link}
{kind=link}
1.0
-
 Health scientists
Health scientists
-
 Report
Report